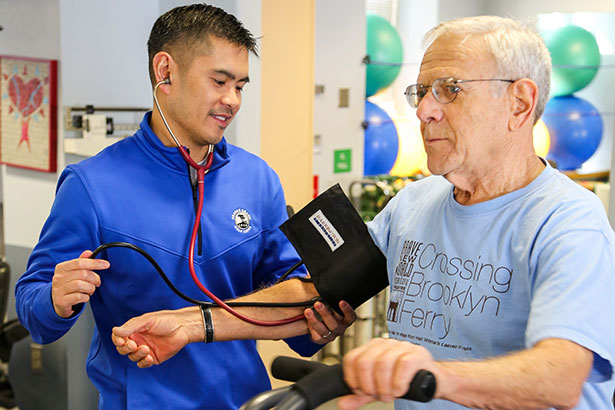
Patients for whom blood transfusion is not an option can still receive comprehensive care at Englewood Hospital and Medical Center, thanks to its pioneering Institute for Patient Blood Management & Bloodless Medicine and Surgery.
The bloodless medicine and surgery program dates to the 1990s, when the institution was approached by Jehovah’s Witnesses who were often denied medical care due to their religious objections to blood transfusions.


“Because we felt that this was such a compelling issue, we assembled key medical and administrative leaders to clearly define clinical, ethical and legal fundamentals for structuring such a program,” said Richard S. Goldweit, MD, section chief of interventional cardiology and medical director of cardiac catheterization laboratory at Englewood Hospital and Medical Center. “We’ve now developed an entire multidisciplinary science to support that effort and manage patients without transfusion.”
Although blood transfusion remains a common part of medical practice in many institutions, it carries a host of clinical and infection-related risks. In addition, transfusions can have negative costs and outcome implications.
“If you look back historically at the literature, the data on blood transfusion are not very good. Transfusions are overused, and there is only a relatively small number of cases where it is actually clinically indicated; most transfusions could be avoided,” Dr. Goldweit said.
In 2000, after observing the early benefits of reducing transfusions, the state of New Jersey partnered with Englewood Hospital to launch an innovative project designed to demonstrate the clinical and public health benefits of bloodless medicine and surgery in patients needing cardiac surgery. Within a few years, Dr. Goldweit and his colleagues published research showing that lowering the transfusion rate in open-heart surgery to 10% improved outcomes by reducing complications and improving survival.
“That 10% transfusion rate is sort of a landmark,” Dr. Goldweit said. “Year after year for more than a decade, Englewood Hospital had a zero mortality rate in cardiac bypass surgery.”
According to evidence documented in the surgical literature, excessive bleeding and vascular complications contribute to poorer outcomes and mortality. Because of this, Dr. Goldweit and his colleagues made the best use of all available technology and developed innovative techniques to avoid transfusions and minimize bleeding whenever possible.
For instance, Dr. Goldweit has developed a bloodless puncture, which consists of routinely working through the radial artery instead of the femoral artery. “Even in patients with myocardial infarction, I can perform a diagnostic angiogram and appropriate stenting procedure through the wrist, which has less bleeding risk.”
He also uses smaller devices to minimize bleeding and is judicious with the use of blood-thinning agents. “We use an intravenous agent that is like Plavix [clopidogrel] but that can be turned off during a procedure if you run into a problem,” Dr. Goldweit explained.
The ongoing success at Englewood Hospital in treating even the most challenging cardiac patients, such as those undergoing high-risk interventional procedures or chronic total occlusion, hinges on the dedication of everyone involved: a collaborative heart team approach.
“The patient blood management program at Englewood is very multidisciplinary. Interventional cardiology is only a small part of it,” Dr. Goldweit said. “We have everybody on the same page, whether they are vascular surgeons or hematologists or gastroenterologists, all trying to limit bleeding, and aggressively treat anemia. Thanks to this approach, we’ve seen many benefits, including improved patient outcomes, shorter hospital stays, less postoperative infections and greater patient satisfaction.”
In addition to publishing research on blood management in cardiac surgery, Englewood Hospital has been extensively involved in the investigation of various devices and therapeutic approaches for treating cardiac patients.
Englewood Hospital is now a participating site in the national ISCHEMIA trial, which is investigating how to best manage people with stable coronary disease, to determine whether medication or more invasive approaches would offer an advantage. “For a community hospital, we’ve enrolled quite a few patients into that trial,” Dr. Goldweit said.
The medical center has also been involved in trials investigating the use of antiplatelet agents in certain stenting platforms. “We’re very much engaged in research, and are now collating our data on TAVR [transcatheter aortic valve replacement] to compare our experience with other sites in New Jersey and nationally,” Dr. Goldweit said.
“Being engaged in research keeps you on the cutting edge,” he added. “It allows you to answer questions you may not have previously had the answers to, especially in situations where you have equipoise and you don’t know which way to go. However, with patient blood management, the benefits are clear.”
Posted September 2017